Skin of color is not the exception. It is the rule.
ROOT & REIGN is for everyone. It is specifically designed for skin of color — roughly 80% of the world’s population — whose biology the industry was never built to serve.

Someone asked me last week if this site is for Asian people.
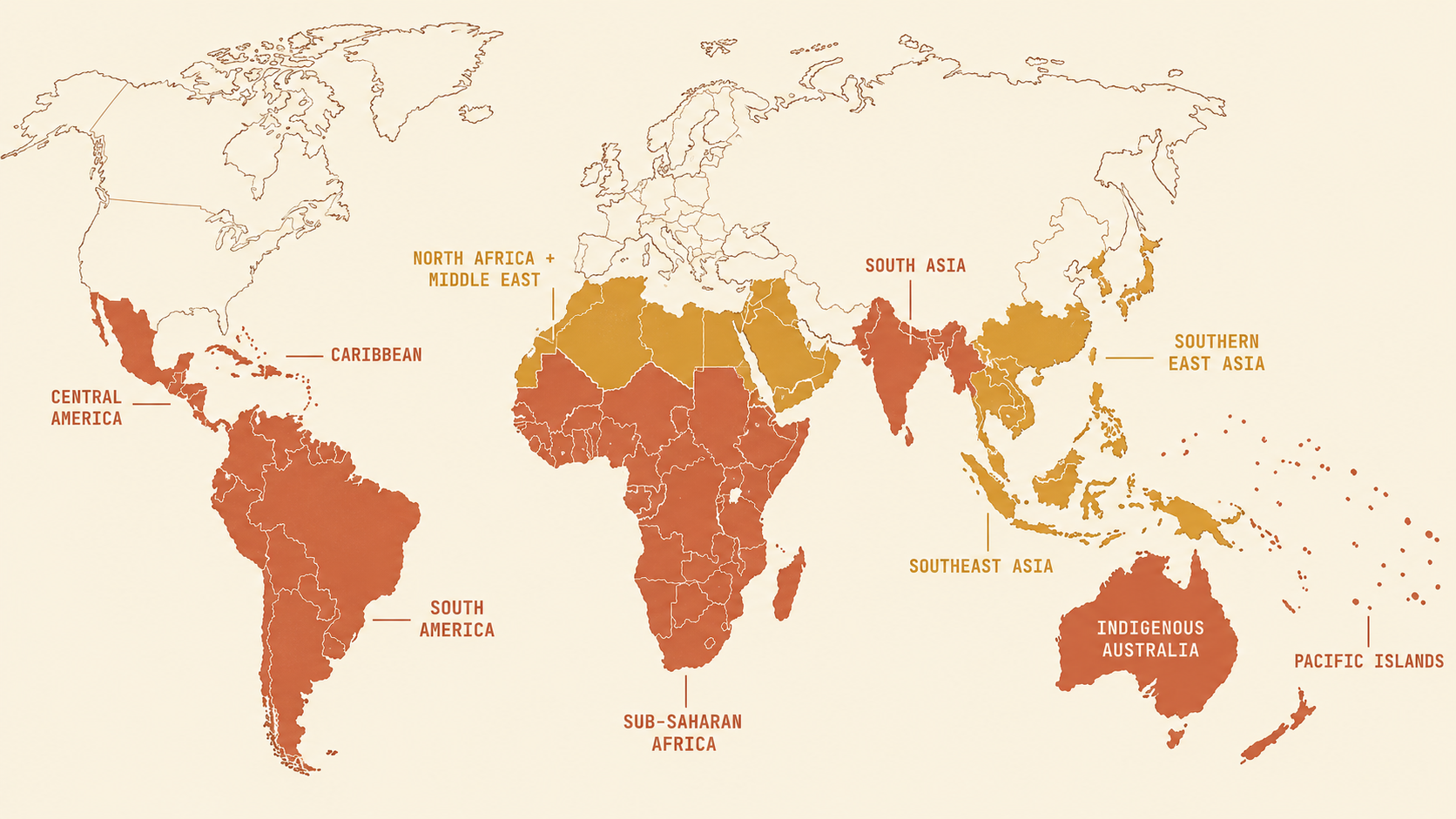
ROOT & REIGN is for everyone. It is specifically designed for skin of color. That means Filipino people, South Asian people — Indian, Pakistani, Sri Lankan, Bangladeshi, Nepali. Indigenous Australians and Torres Strait Islander communities. Most Latina and Latinx people, depending on your ancestry and how it moved through your bloodline. People of African descent across the diaspora — on the continent, in the Caribbean, in the United States, in the United Kingdom, in Brazil. Southeast Asians: Vietnamese, Thai, Indonesian, Malaysian, Cambodian. Pacific Islanders. Many East Asian populations, particularly those with deeper complexions. Middle Eastern and North African communities where hyperpigmentation and melasma are among the most common presenting dermatological concerns. Add all of those people up and you get roughly 80% of the world. ROOT & REIGN was built for the majority.
Skin of color is not a demographic. It is a biological category.
The clinical term does not mean Black skin. It does not mean African skin. It refers to skin with elevated melanin density — skin whose melanocytes produce more pigment, distribute it more broadly through the skin's layers, and respond more forcefully when the skin is injured or inflamed. That biology is not unique to one community. It runs through most of the world. In 2026, an international expert consensus panel — dermatologists from China, South Africa, Brazil, India, and the United States — published a formal call to redefine how medicine approaches skin of color. Their consensus paper noted that the existing definition "is often used simply to denote individuals who are not of Caucasian White origin" and documented that clinical trials, dermatology education, and diagnostic tools still fail to represent these populations at anything close to their global prevalence. That is not a research gap. That is a choice that has been made, repeatedly, for decades.
One mechanism. Many populations.
When skin with elevated melanin density experiences inflammation — a breakout, a razor bump, a wound, a rash, a chemical irritation — the melanocytes at the site of injury produce more pigment than the healing requires. The immune system calls for melanin as part of wound response. On lighter skin, the process resolves relatively quickly and the mark fades. On skin with higher melanin density, the mark persists — sometimes for months, sometimes for years. This is postinflammatory hyperpigmentation. It is not a disease. It is not a sign that your skin is damaged or reactive in some exceptional way. It is what happens when skin built with more melanin does its job. That mechanism operates identically across every population with elevated melanin density. The melasma that disproportionately affects South Asian women — amplified by hormonal changes during pregnancy, exacerbated by UV exposure — traces back to the same biological pathway as post-acne hyperpigmentation on Black skin. The dark marks that remain after eczema flares in Filipino and Indonesian teenagers come from the same cascade. The persistent hyperpigmentation after insect bites in Indigenous communities across the tropics is the same wound-healing overshoot, on the same melanocyte-dense skin. One mechanism. Dozens of communities. One body of research, built almost entirely on populations for whom this mechanism rarely presents as a serious concern.
Colorism is the connective tissue.
There is a practice that appears in West Africa and South Asia and the Philippines and Brazil and the Caribbean and East Africa and South Korea. Communities separated by thousands of miles, different histories, different languages, different religions. All of them developed markets for products that promise to lighten skin. All of them normalized the pursuit of a complexion closer to the colonial standard. Some people discuss this as if each community arrived at the practice independently — as if there is something in the culture, or in the psychology, or in some particular self-perception, that explains why it took hold there. That explanation is wrong. Skin lightening is popular in Lagos and Mumbai and Manila and São Paulo for the same reason. Colonialism installed a hierarchy that made lighter skin the visible marker of status, safety, and proximity to power — and it did this across every territory it touched, at roughly the same historical moment. The communities are different. The mechanism is the same. It was not arrived at independently across cultures. It was installed. The industry that refused to develop products for skin of color's actual biology was simultaneously building and marketing products that promised to bring skin of color closer to a standard it had invented. The harm from those products — mercury in unregulated brightening creams, hydroquinone at dangerous concentrations sold over the counter, unlabeled prescription-strength corticosteroids in bleaching creams distributed across markets where regulatory oversight is limited — falls on the same populations that mainstream dermatology was failing to study. That is not irony. That is a system.
The research was built for 20% of the world.
The most commonly used severity scales in inflammatory dermatology rely on erythema — redness — as the primary assessment marker. These tools were developed and validated on Fitzpatrick I through III skin. On darker skin, redness either does not appear visibly or presents differently. A 2025 paper documented this failure directly: patients with skin of color are systematically underdiagnosed or misclassified by tools that were never designed to see their presentations clearly. This is the scope of the gap. It is not only which populations get enrolled in clinical trials. It is whether the basic diagnostic infrastructure of dermatology was built to correctly identify what is happening in skin of color patients at all. Certain genetic variations are common in specific populations — variations that affect how skin and hair behave, how sweat glands function, how bodies respond to particular environmental exposures — that the personal care industry has never designed around because the populations carrying them were never considered the target market. The absence of those products is not accidental. It reflects the same assumption that shaped the clinical research: that the default human is lighter-skinned, and that everyone else is the variation.
What ROOT & REIGN is for.
This site exists because the assumption is backward. The products, the research, the diagnostic tools, the "dermatologist recommended" language on packaging — all of it was calibrated for a minority of the world's population. The rest of the world, roughly 80% of it, has been told to use those products anyway, to adapt the advice that was not written for their skin, to manage on their own the conditions the research was not designed to study. ROOT & REIGN's evaluator is built on a single correction: your skin's biology should be the operating assumption, not the afterthought. The mechanisms that drive hyperpigmentation — the five pathways that produce postinflammatory marks — are not African pathways or Asian pathways. They are the pathways of skin built with more melanin. The evaluator reads your products against what the research actually says about those pathways, for the Fitzpatrick types those pathways most directly affect. That is most of the world. It is time the tools reflected that. Ready to evaluate what is in your current routine? Bring your ingredient list to the ROOT & REIGN evaluator. It reads your products against what the research actually says — calibrated for skin built with more melanin, because that is most of the world, and it is time the tools reflected that. Reign in Your Skin.

The routine is the remedy. Read the ingredient list, then make the choice that works with your skin.
Skin of color isn’t a niche or a single ethnicity — it’s a biological category: skin with more melanin, which answers any irritation by making extra pigment. That describes roughly 80% of the world, from the African diaspora to South and Southeast Asia, Latin communities, Indigenous and Pacific peoples, and more. The same pigment mechanism runs through all of them, yet most dermatology research, products, and even diagnostic tools were built on the other 20% with lighter skin. The skin-lightening pressure many of these communities feel wasn’t invented separately in each place; colonialism installed the same hierarchy everywhere it reached. ROOT & REIGN is built on the opposite assumption: your skin’s biology is the default to design for, not the exception.
Reign in your skin
ROOT & REIGN is for everyone. It is specifically designed for skin of color — roughly 80% of the world’s population — whose biology the industry was never built to serve.
Evaluate your products →Doctor Djeli is an educational resource, not medical advice.