
You are reaching for the wrong thing.
Every wound on skin of color is a PIH event in waiting.
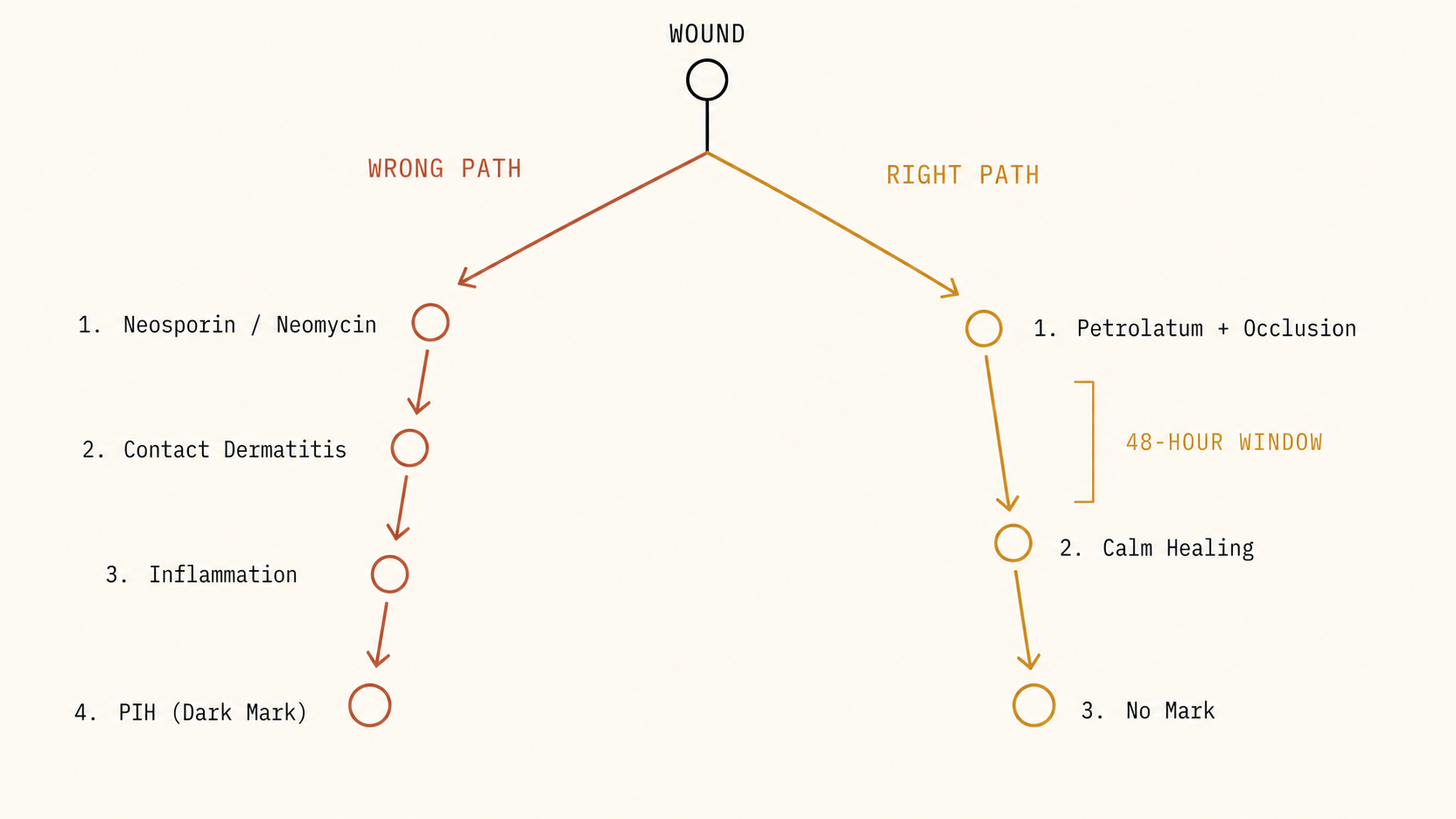
Every cut, every scrape, every shaving nick on skin of color is a PIH event in waiting. The dark mark does not come from the wound. It comes from the inflammatory cascade the wound triggers — and that cascade begins within hours of the injury, long before the skin closes. What you reach for in the first 48 hours determines what your skin looks like in six months. Most people reach for the wrong thing.
On skin with elevated melanin density, any inflammatory signal — including the normal wound-healing response — instructs melanocytes to overproduce pigment. On lighter skin, the mark fades in weeks. On Fitzpatrick IV through VI skin, that mark can take months to years to resolve, if it resolves at all. This means wound management on skin of color is not just first aid. It is PIH prevention.

Every cut, every scrape, every shaving nick on skin of color starts a cascade. What you reach for in the first 48 hours determines what your skin looks like in six months.
The product you reach for first may be generating the exact inflammation that leaves the mark.
Neosporin has three active ingredients: neomycin, polymyxin B, and bacitracin. Neomycin — the N in the name — is one of the most common contact allergens in clinical dermatology. Consistent use on wounds causes allergic contact dermatitis in a meaningful percentage of people. Allergic contact dermatitis is inflammation. Inflammation on skin of color is a PIH trigger.
The same product you are applying to prevent infection is, for many people, generating the exact inflammatory response that turns a minor cut into a months-long dark mark.
For clean minor wounds — the kind most people are treating at home — the antibiotic component is not what matters. Occlusion is what matters. And petrolatum does that job without any sensitization risk. The instinct to let a wound air out and dry is also wrong. Moist wound healing — keeping the wound site covered and occluded — accelerates re-epithelialization by roughly 50% compared to air-drying. The scab that forms over a dried wound is not a sign of healing. It is a barrier the skin has to work through rather than with.
The inflammatory cascade begins within hours. The first 48 hours determine the outcome.

The scab is not a sign of healing. It is a barrier your skin has to work through rather than with.
Petrolatum. Panthenol. Hypochlorous acid. Hydrocolloid bandages.
Petrolatum. Plain petroleum jelly — the correct first-reach for any minor wound. No fragrance, no sensitizers, no mechanism that generates inflammation. Creates a moist occlusive environment while the skin heals underneath. Available for under two dollars.
Panthenol healing balm. Any product whose first actives are panthenol and a simple occlusive base. Panthenol — provitamin B5 — actively promotes re-epithelialization rather than just occluding. The ingredient function is what matters, not the brand.
Hypochlorous acid (HOCl). When a wound needs antimicrobial coverage beyond petrolatum’s occlusion, HOCl is the correct choice. It is the antimicrobial the immune system already produces. Anti-inflammatory while it is antimicrobial — it does not add to the inflammatory load at the wound site. It does not cause contact dermatitis. Apply it, then follow with petrolatum and an occlusive bandage.
Hydrocolloid bandages. The same technology behind acne patches. They maintain a moist wound environment actively, protect from environmental bacteria, and are better than standard gauze for minor cuts and scrapes. What does not belong: Neosporin. Hydrogen peroxide. Rubbing alcohol. Anything that stings — stinging means tissue damage, which means inflammation, which means PIH.
Four phases. The 48-hour window decides the PIH outcome. The months after decide the scar.
- Immediate
Petrolatum or panthenol healing balm + occlusive bandage
Clean the wound with water only. Apply petrolatum or panthenol balm. Cover with an occlusive or hydrocolloid bandage. Keep it covered until the wound closes.
- Antimicrobial
HOCl if contamination is a concern
Hypochlorous acid provides antimicrobial coverage without the tissue damage, contact dermatitis, or PIH risk of hydrogen peroxide, alcohol, or neomycin-containing products.
- Once closed
Silicone gel twice daily — or sheeting 8–12 hrs/day
The most validated OTC scar prevention intervention. Applied consistently to the closed wound over weeks to months, it modulates collagen production and prevents hypertrophic scar formation.
- After — PIH
Niacinamide + azelaic acid + TXA + vitamin C
The brightening actives address the residual dark mark. None of these is a one-week fix. All of them work if used consistently. The routine is the remedy.
If you missed the window — the mark is not permanent. The routine is still the remedy.
If you did not manage the wound correctly — if you reached for Neosporin, if you air-dried it, if the window passed before you knew it mattered — the mark is not permanent. Postinflammatory hyperpigmentation from old wounds fades with the same actives that address any hyperpigmentation on skin of color. Niacinamide blocks the transfer of melanin from where it is produced to where it becomes visible. Azelaic acid inhibits the enzyme that produces melanin. Tranexamic acid works upstream, intercepting the inflammatory signal before it instructs melanocyte activation. Vitamin C derivatives provide antioxidant coverage that dampens the free radical load driving continued melanin overproduction.
None of these is a one-week fix. All of them work if used consistently. What you do every day over time is what changes what your skin looks like. The routine is the remedy.

The mark is not permanent. The actives are probably already in your cabinet. Use them consistently, and let the biology catch up.
Evaluate Your Products → Not sure what you’re using? Evaluate it →
Reign in your skin
Doctor Djeli is an AI, trained on evidence-based dermatology and lived expertise in melanated skin — built by a real person who navigated this firsthand. Educational resource, not medical advice.