
It works. It also carries the highest risk on skin like yours.
The most clinically proven topical depigmenting agent — and the highest-risk brightener for this skin.
Hydroquinone is the most clinically proven topical depigmenting agent in the dermatology literature. It is also the brightener with the highest risk profile on Fitzpatrick IV–VI skin specifically, and the most-abused active ingredient in skin lightening culture worldwide. These two facts are both true at the same time. The honest treatment requires holding both.
This article will not tell you hydroquinone is dangerous and to never go near it. The clinical research on appropriate, supervised use shows it works. This article will also not tell you hydroquinone is the answer to your hyperpigmentation. The risk profile on melanated skin specifically makes it a tool to use carefully, with medical supervision, in defined situations, for defined durations — not a daily skincare product, and not a permanent fixture in a routine.

The honest position is not “avoid it” and not “use it.” Know exactly when it is the right tool and when it is the most dangerous one in the cabinet.
Hydroquinone blocks tyrosinase AND reduces the melanocyte population. That is why it works fast — and why the risks exist.
Hydroquinone is a tyrosinase inhibitor that works in two ways: it blocks the enzyme directly, and it is cytotoxic to melanocytes themselves at therapeutic concentrations, reducing the number of melanocytes producing pigment in the treated area. This is why it works fast compared to most other brighteners — you are not just reducing melanin production; you are reducing the melanocyte population that produces it.
The cytotoxic action that makes it effective in the short term is the same action that produces the more serious adverse effects with prolonged use.
For melasma at 4% hydroquinone cream, the published evidence is unambiguous. Twelve to twenty-four weeks of consistent use produces meaningful reduction in MASI scores, with effect sizes that outperform most over-the-counter brighteners. The “Kligman formula” — hydroquinone 4% combined with tretinoin 0.05% and dexamethasone 0.01% — remains one of the most-prescribed depigmenting protocols for moderate-to-severe melasma in dermatology practice. The efficacy is real. The mechanism is well-understood. The clinical evidence base is extensive.
Short course, dermatologist-prescribed, monitored. The serious risks appear in years of unsupervised use — not in properly managed courses.
Ochronosis, paradoxical hyperpigmentation, and skin atrophy — all disproportionate on Fitzpatrick IV–VI.
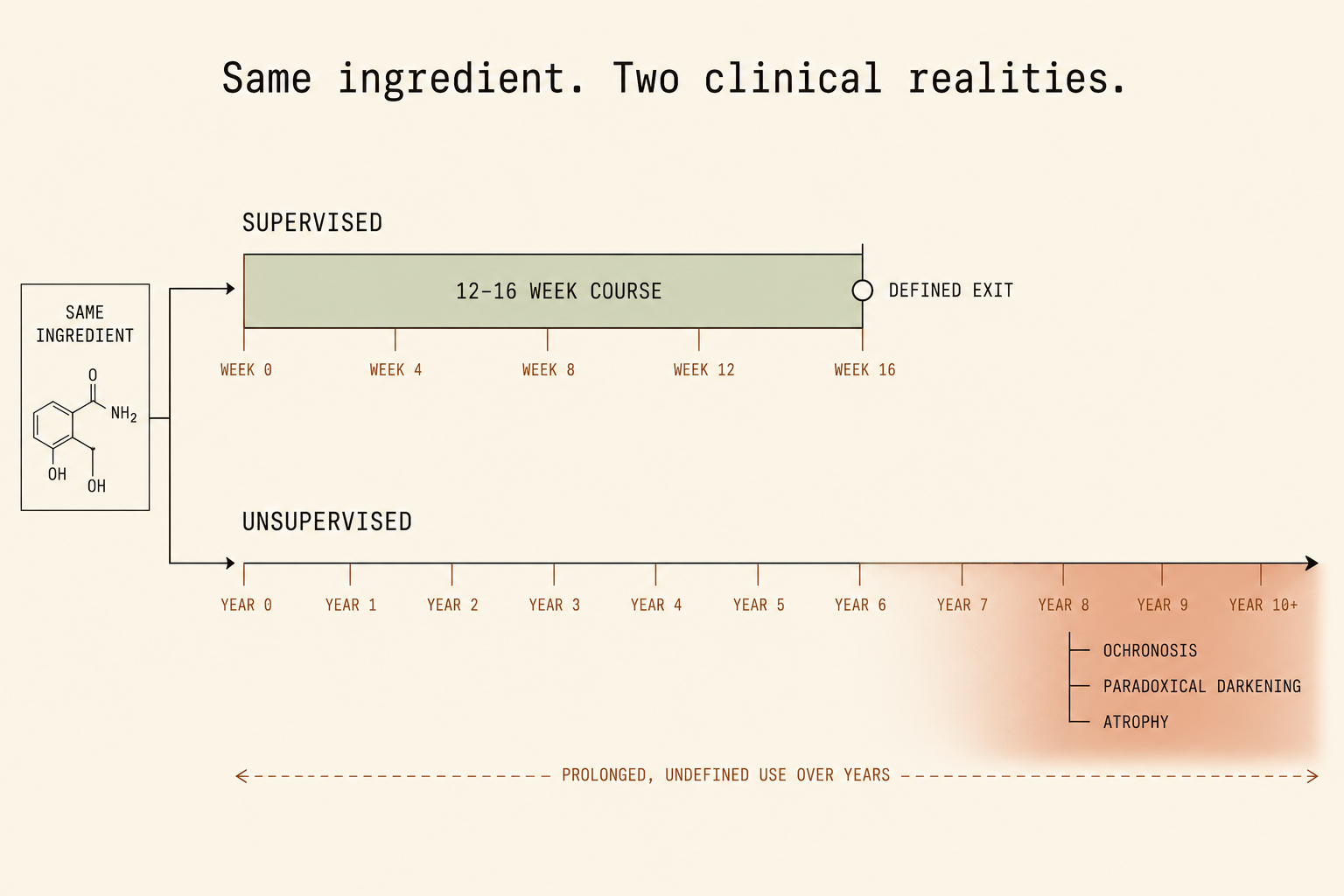
Ochronosis is a paradoxical pigmentation disorder that produces a blue-black-gray discoloration of the skin, associated with prolonged hydroquinone use (often years) at higher concentrations (5%+), and disproportionately affects Fitzpatrick IV–VI skin. Once ochronosis develops, it is extremely difficult to reverse — meaningfully more difficult than treating the original PIH.
Paradoxical hyperpigmentation is distinct: the skin responds to prolonged hydroquinone use by producing more pigment, not less. The treatment, used wrong, can produce a darker face than the user started with. Skin atrophy and chronic irritation occur at higher rates on darker skin from prolonged exposure. These adverse effects do not appear in 4-week prescription courses. They appear in years of unsupervised use. The distinction matters more than almost anything else in this conversation.

Ochronosis. Paradoxical darkening. Skin atrophy. All disproportionate on deeper skin. All appearing in years of unsupervised use — not in properly monitored courses.
Prescribed clinical use and unsupervised skin lightening use share an ingredient. They share nothing else.
Hydroquinone at high concentrations (5–10%+), often combined with mercury salts or potent topical corticosteroids, is the active in a global skin lightening industry that exists entirely outside of medical supervision. The harms documented in this context are not speculative: ochronosis, severe atrophy, corticosteroid-related complications from contaminated products. This is not the same as a dermatologist prescribing 4% hydroquinone for a 12-week melasma course with periodic monitoring. The two use patterns share an active ingredient and otherwise have very little in common.
The framework here treats prescribed clinical use as one thing and unsupervised lightening use as another. The first is a defensible clinical tool used appropriately. The second is harm dressed as skincare.
Know exactly when to reach for it and when not to.
- First line
Give the lower-risk brighteners 12 weeks first
Azelaic acid + niacinamide + TXA + vitamin C derivative, at full therapeutic concentration, consistently used. Most of the time the honest answer is that this protocol has not been properly run yet.
- Escalation
Prescription only — 4%, 12–16 week course, monitored
Moderate-to-severe melasma that has not responded to first-line agents after 12+ weeks of proper use. Dermatologist-prescribed and monitored, with a defined exit date.
- Severe
Kligman formula — specialist in skin of color
Hydroquinone 4% + tretinoin 0.05% + dexamethasone 0.01%. Dermatologist-prescribed, monitored, defined duration. Find a provider who specializes in Fitzpatrick IV–VI skin.
- Avoid
OTC products with no clear concentration or duration
Any hydroquinone product marketed for general “brightening” without a defined course, any product combining hydroquinone with mercury or potent corticosteroids, and any prolonged unsupervised use past 16 weeks.
Two specific scenarios — both require a dermatologist, both require a defined exit.
Hydroquinone has a place in a melanated-skin PIH protocol in two specific scenarios. The first is moderate-to-severe melasma that has not responded to the lower-risk brighteners used appropriately for at least 12 weeks. In that context, a dermatologist-prescribed 4% course, limited to 12–16 weeks with periodic monitoring for adverse effects, is an evidence-based escalation. The second is the Kligman formula or similar combination protocol for severe melasma — again dermatologist-prescribed, monitored, with a defined duration.
For routine PIH on Fitzpatrick IV–VI skin, the better question is whether the lower-risk brighteners have had 12 weeks at full therapeutic concentration with consistent use. Most of the time, the honest answer is no — and the appropriate next step is to actually run that protocol, not escalate to a higher-risk option that may produce a worse outcome than the original problem.

Before you escalate, ask honestly: have the lower-risk brighteners had 12 weeks at full concentration? Most of the time, the honest answer is no.
Evaluate Your Products → Not sure what you’re dealing with? Evaluate it →
Reign in your skin
Doctor Djeli is an AI, trained on evidence-based dermatology and lived expertise in melanated skin — built by a real person who navigated this firsthand. Educational resource, not medical advice.