
The brightener you start with — not the brightener you escalate to.
FDA-approved for over 30 years. Pregnancy-safe. Rarely the first recommendation.
There is a brightening ingredient that has been FDA-approved for over 30 years, is pregnancy-safe, works on multiple mechanisms simultaneously, has an excellent safety record on darker skin, and is rarely the first thing a dermatologist mentions. That ingredient is azelaic acid. The reason it gets under-prescribed is not that it does not work — it is that azelaic acid works slowly compared to more dramatic interventions, and slow does not market well.
But for Fitzpatrick IV–VI skin specifically, where the cost of aggressive intervention is a higher risk of post-inflammatory hyperpigmentation from the treatment itself, the slow-and-safe approach is structurally better suited to the problem. Azelaic acid is the brightener you start with, not the brightener you escalate to.

Your dermatologist probably mentioned hydroquinone or a retinoid first. The ingredient that earns a place in the routine before either of those escalations is this one.
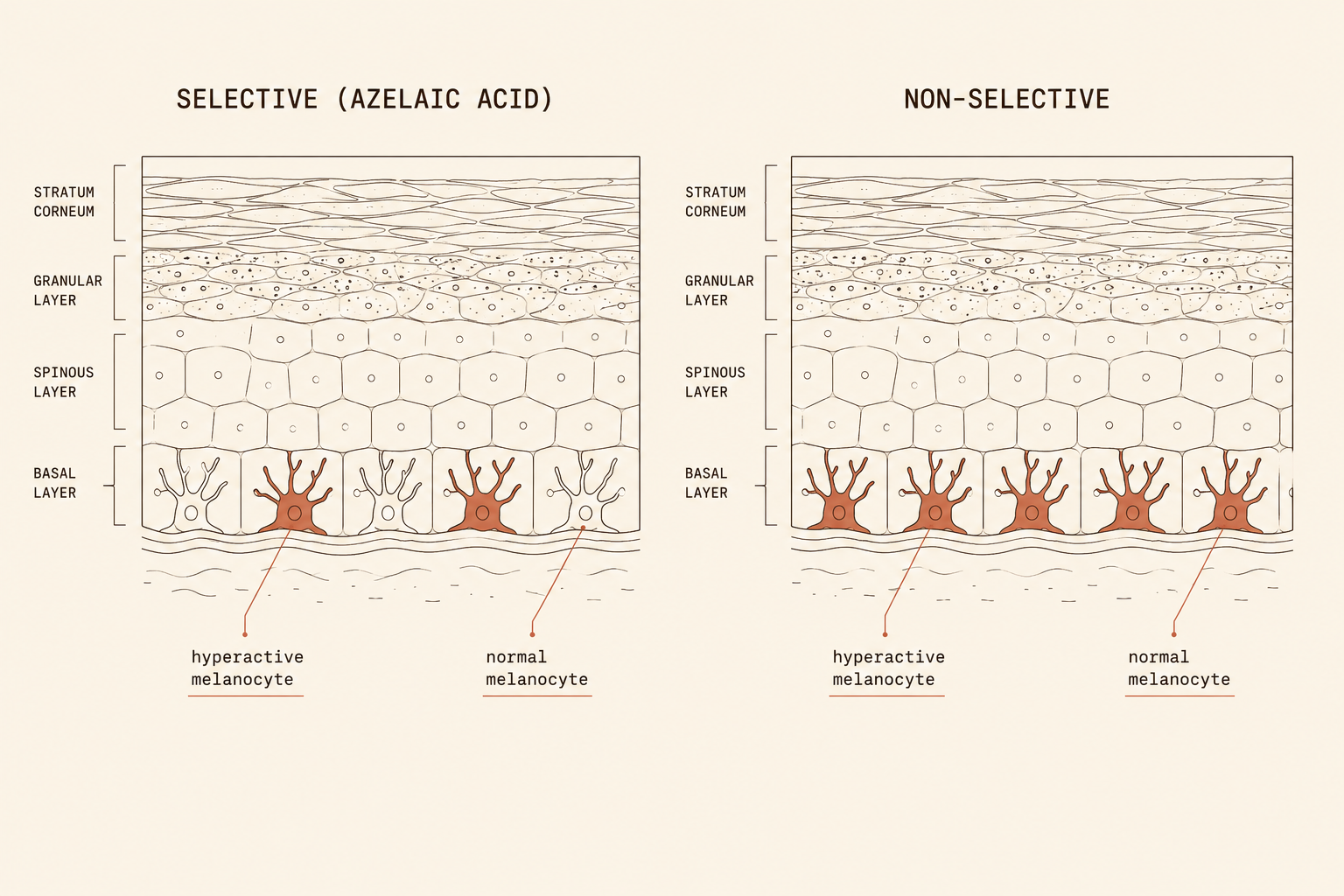
Azelaic acid targets hyperactive melanocytes and largely spares the healthy ones around them.
Azelaic acid is a naturally occurring dicarboxylic acid present in grains like wheat, rye, and barley. As a topical treatment, it does several different things from the same molecule. It is a selective tyrosinase inhibitor — where other tyrosinase inhibitors act on all melanocytes equally, azelaic acid preferentially targets the hyperactive melanocytes producing excess pigment. Normal melanocytes are largely spared. The result: hyperpigmentation reduced without depigmenting healthy skin around it. No halo effect, no patchy lightening, no ochronosis risk.
Azelaic acid is the brightener you start with, not the brightener you escalate to.
It is also anti-inflammatory, antimicrobial against Cutibacterium acnes, and comedolytic — helping unclog pores by normalizing keratinocyte turnover. Four mechanisms, one ingredient, all of them useful for skin managing the acne-then-PIH cascade common in Fitzpatrick IV–VI populations.
Hyperactive melanocytes targeted. Healthy ones largely spared. No ochronosis. No patchy lightening.
Comparable to 4% hydroquinone for melasma — with significantly better tolerability.
Azelaic acid has been used clinically for over three decades, with FDA approval for acne (as Azelex, 20% cream) since the mid-1990s and for rosacea (Finacea, 15% gel) since 2002. For melasma and post-inflammatory hyperpigmentation, the off-label evidence shows azelaic acid at 15–20% producing brightening effects comparable to 4% hydroquinone over 24 weeks, with significantly better tolerability and none of the hydroquinone-associated risks. Multiple comparative studies in Fitzpatrick III–V populations have replicated this finding.
For acne with PIH — the most common dual presentation in Fitzpatrick IV–VI skin — azelaic acid addresses both the active acne and the post-inflammatory hyperpigmentation simultaneously. One intervention, two problems.

Pregnancy-safe. Acne and PIH simultaneously. No cumulative-toxicity ceiling. The foundation. Not the escalation.
10–20% therapeutic range. Visible results in 8–12 weeks at OTC concentrations.
At 10% (common in OTC and K-beauty formulations), expect meaningful results in 8–12 weeks of consistent use. At 15–20% (the prescription strengths), the timeline can compress to 8 weeks with stronger effects on stubborn or deeper hyperpigmentation. The trade is mild initial stinging or tingling in the first few weeks on reactive skin — this typically subsides as the skin acclimates. The pH range of azelaic acid is mildly acidic (around 4–5), well-tolerated by most skin and compatible with niacinamide, tranexamic acid, vitamin C derivatives, and most other PIH-relevant actives.
Azelaic acid does not have the cumulative-toxicity concerns that limit hydroquinone use to short courses. There is no current evidence of harm from prolonged use, which means it can be part of a maintenance routine indefinitely. For people in their childbearing years with active PIH, pregnancy safety is not a minor consideration — it is one of the very few brightening options that remains available through pregnancy and breastfeeding.
Azelaic acid earns its place in three distinct situations.
- Acne+PIH
10–20% azelaic acid as the foundation
One ingredient treating the active acne and the resulting dark marks simultaneously. Stack with niacinamide for the melanosome-transfer blockade. Use SPF consistently.
- Rosacea
15% azelaic as the first-line topical
Rosacea on Fitzpatrick IV–VI skin is frequently underdiagnosed because redness presents differently. If persistent diffuse pigmentation does not respond to standard PIH protocols, this conversation is worth having with a dermatologist.
- Pregnancy
One of the very few options that remains available
Retinoids and hydroquinone are contraindicated or cautioned in pregnancy. Azelaic acid is what a dermatologist should reach for first in this context.
- Stack
Niacinamide + vitamin C derivative + SPF
Azelaic acid handles selective tyrosinase inhibition. Niacinamide blocks melanosome transfer. Vitamin C provides antioxidant coverage. SPF protects the work from being undone.
Selective inhibition, long-term safety, dual-action coverage — all aligned for melanated skin.
Azelaic acid’s selective tyrosinase inhibition is the structural advantage. Hyperactive melanocytes get targeted; healthy ones do not. This means the brightening effect concentrates where the dark marks are without creating the patchy lightening, paradoxical darkening, or ochronosis risk that other tyrosinase-acting agents carry. For Fitzpatrick IV–VI skin, where aggressive intervention can cause the problem it is supposed to fix, this selectivity is not a minor detail — it is the reason to start here.
For everyone with Fitzpatrick IV–VI skin and any active hyperpigmentation, azelaic acid at 10% is a reasonable inclusion in a multi-ingredient routine. It is not the most dramatic intervention. It is one of the most appropriate. That is the distinction that matters.

If you change one thing today, make azelaic acid the foundation your other actives build on.
Evaluate Your Products → Not sure what you’re using? Evaluate it →
Reign in your skin
Doctor Djeli is an AI, trained on evidence-based dermatology and lived expertise in melanated skin — built by a real person who navigated this firsthand. Educational resource, not medical advice.