
Every other brightener stops the enzyme. This one stops the instruction.
Tranexamic acid does not block tyrosinase. It works upstream of it.
If you have been reading about hyperpigmentation treatment for any length of time, the conversation has been about tyrosinase. Vitamin C inhibits it. Niacinamide blocks the transfer of what it makes. Kojic acid chelates the copper at its active site. Hydroquinone interferes with it directly. The mechanism has been the same shape for decades — find the enzyme that makes melanin and stop it.
Tranexamic acid is the rare ingredient that does not do any of that. Instead of stopping the production of melanin, it stops the instruction to produce more melanin from ever being sent. This is not marketing language. It is a specific biological pathway, and it is why tranexamic acid has emerged in the dermatological literature as one of the most appropriate brightening interventions for Fitzpatrick IV–VI skin specifically.

Vitamin C, niacinamide, kojic acid — all of them act downstream. Tranexamic acid intercepts before the melanocyte ever gets the signal to produce.
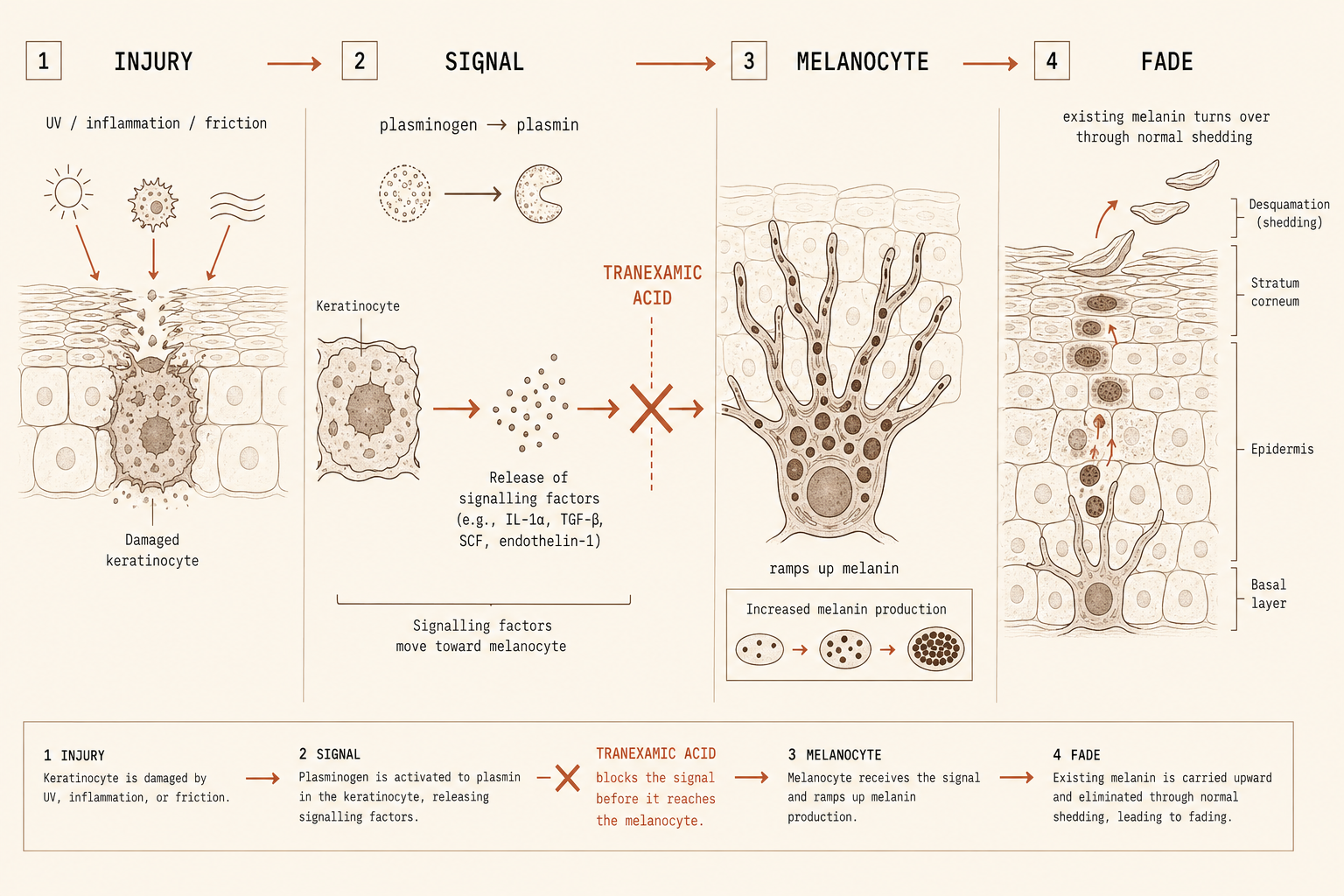
When skin is injured, keratinocytes activate a pathway. Tranexamic acid blocks that pathway.
When skin is injured — by inflammation, UV exposure, friction, an active breakout, a shave that went wrong — damaged keratinocytes release signaling molecules that activate the plasminogen-plasmin system. This is the same system the body uses to manage blood clotting. In the skin, when this pathway activates, the keratinocytes start producing factors that travel to nearby melanocytes and instruct them to ramp up melanin production. This is the inflammatory cascade that produces post-inflammatory hyperpigmentation.
This is the mechanism distinction that makes tranexamic acid different in kind, not just in degree, from every other brightener on the market.
Tranexamic acid is an antifibrinolytic agent — its job is to inhibit plasminogen activation. In the skin, that activity intercepts the keratinocyte-to-melanocyte conversation before the signal to make more pigment ever reaches the melanocyte. The melanin that is already there continues to turn over and fade through normal cell shedding, but the cascade that produces new melanin is interrupted at the source.
Injury signals the keratinocyte. The keratinocyte instructs the melanocyte. Tranexamic acid stops the instruction before it arrives.
Trials conducted in Fitzpatrick III–V skin-of-color populations — closer to your biology than most dermatology data.
The bulk of clinical literature on tranexamic acid for hyperpigmentation was conducted in Fitzpatrick III–V skin-of-color populations. The numbers are not subtle. A randomized controlled trial of oral tranexamic acid at 250mg twice daily for three months produced a 49% reduction in mMASI score, versus an 18% reduction in the placebo group. A 3% topical formulation showed efficacy comparable to a 3% hydroquinone protocol — with no detectable systemic absorption.
Studies combining higher topical concentrations with microneedling showed more dramatic results: one trial of 10% tranexamic acid delivered via microneedling produced a 65.92% improvement in mMASI scores at 8 weeks, compared to 20.75% with microneedling alone. For post-inflammatory hyperpigmentation, the mechanism translates directly — any condition where the inflammatory cascade drives the pigment response is within tranexamic acid’s range.

For skin where every inflammatory event becomes a dark mark, upstream is the answer. The mechanism aligns with the biology.
Two routes, two clinical conversations.
Oral tranexamic acid (typically 250mg twice daily for melasma, 650mg daily for short-term PIH prevention) has the strongest evidence base. It is also a systemic medication with real contraindications: hypercoagulable conditions or active bleeding, history of thromboembolic disease, renal impairment, pregnancy, breastfeeding, and concurrent hormone therapies including oral contraceptives. A recent meta-analysis found no increased thromboembolic risk in non-surgical patients without these underlying risk factors. Oral TXA is a prescription conversation with a dermatologist — and one worth having if you fall outside the contraindication list.
Topical tranexamic acid at 2–5% reaches the upper layers of the skin where keratinocyte signaling is happening. A 3% topical formulation has been shown not to produce detectable systemic absorption. It can be combined safely with vitamin C, niacinamide, and azelaic acid — the mechanisms are non-overlapping, which means the brightening interventions stack rather than compete.
The intervention that closes a specific gap. Stack it with what you already have.
- Active PIH
Topical TXA at 2–5%
The upstream intervention. Intercepts the inflammatory signal before it reaches the melanocyte. Use it alongside, not instead of, the rest of your brightening stack.
- Stack
Vitamin C + niacinamide + azelaic acid
Mechanisms are non-overlapping: TXA intercepts the signal, vitamin C inhibits tyrosinase, niacinamide blocks transfer, azelaic acid targets hyperactive melanocytes. They compound.
- Hormonal
Melasma: ask about oral TXA
The strongest evidence-based topical option for hormonal hyperpigmentation. The oral prescription conversation is worth having with a dermatologist if topical is insufficient.
- Reactive
For skin that flares with actives
Tranexamic acid is one of the few brighteners with a safety profile appropriate for skin that cannot tolerate most brighteners. No serious adverse skin reactions in published trials.
The safety profile, the evidence stack, and the mechanism all align for melanated skin.
Fitzpatrick IV–VI skin’s central problem is the reactivity of the inflammatory cascade. Any injury produces a melanin response. The brighteners that work by blocking tyrosinase are acting after the cascade has already fired — reducing the volume of melanin produced, but not preventing the cascade itself. Tranexamic acid intervenes before the cascade fires. For skin where the cost of any inflammatory event is a new dark mark, that mechanism is structurally better suited to the problem.
The safety profile matters too. Vitamin C at the concentrations required for direct potency can irritate. Retinoids cause inflammatory shedding. Hydroquinone has its ochronosis risk, which falls disproportionately on darker skin. Topical tranexamic acid does not have these liability patterns — it is well-tolerated even on reactive skin. The mechanism aligns with the biology. The evidence was run in skin-of-color populations. The safety profile holds.

If you are managing active PIH — post-acne marks, razor bump darkening, dark marks from any inflammatory event — tranexamic acid is one of the most mechanism-appropriate ingredients available.
Evaluate Your Products → Not sure what you’re dealing with? Evaluate it →
Reign in your skin
Doctor Djeli is an AI, trained on evidence-based dermatology and lived expertise in melanated skin — built by a real person who navigated this firsthand. Educational resource, not medical advice.